Peritoneal Dialysis
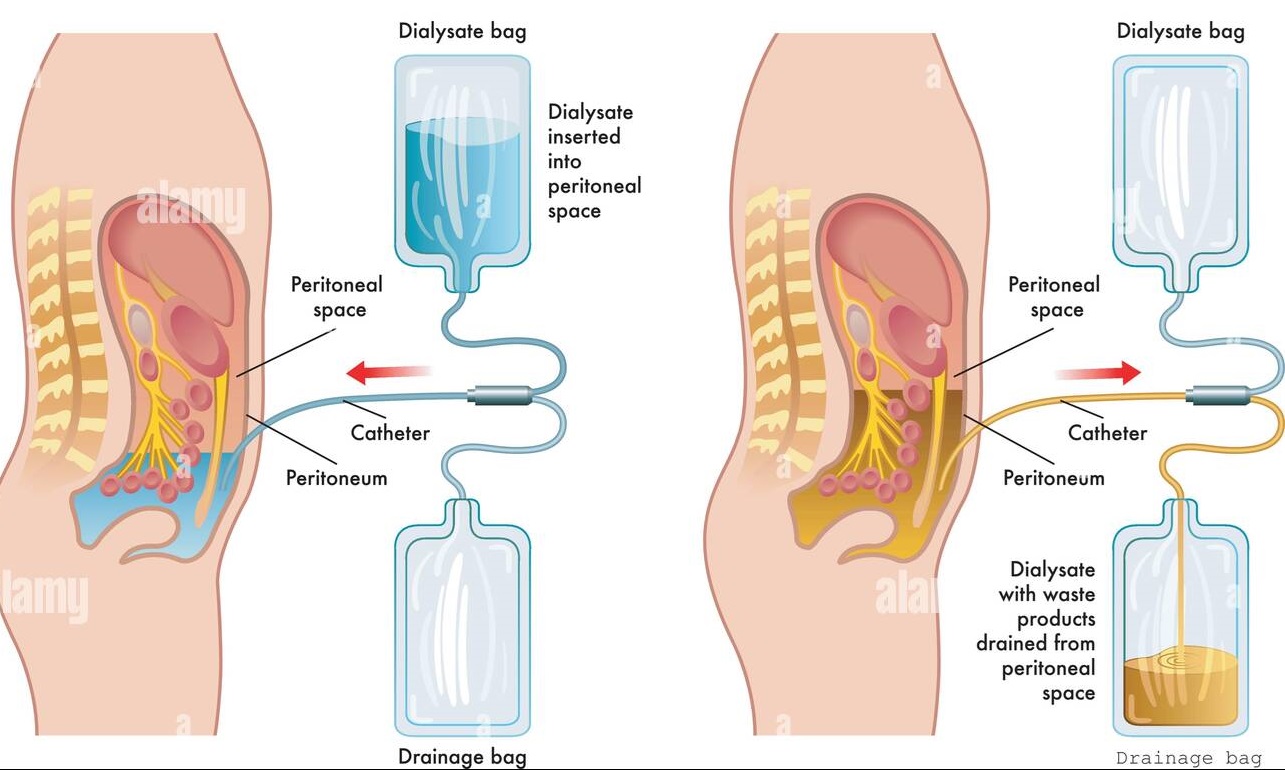
Peritoneal dialysis (PD) is a treatment for patients with severe chronic kidney disease. The process uses the patient’s peritoneum in the abdomen as a membrane across which fluids and dissolved substances are exchanged from the blood. Fluid is introduced through a permanent tube in the abdomen and flushed out either every night while the patient sleeps (automatic peritoneal dialysis) or via regular exchanges throughout the day (continuous ambulatory peritoneal dialysis). PD is used as an alternative to haemodialysis though it is far less commonly used in many countries. It has comparable risks but is significantly less costly in most parts of the world, with the primary advantage being the ability to undertake treatment without visiting a medical facility. The primary complication of PD is infection due to the presence of a permanent tube in the abdomen. In this technique the peritoneum and vessels act as dialysis
Types of Peritoneal Dialysis (PD)
Intermittent peritoneal dialysis (IPD)
It is usually performed with hourly exchanges of 2 liters of dialysate and continued for 48-72 hours. In can be done manually or by automatic apparatus. This techniques is of only limited usefulness in intensely catabolic patients and in cases of drug intoxication. This technique provides a temporary urea clearance of approximately 20 ml / minute.
Continuous ambulatory peritoneal dialysis (CAPD)
In this technique a 2 liter exchange is performed by the patient 4 times daily. 2 liters of commercial dialysate fluid contained in a soft plastic bag runs into the peritoneal catheter. The empty bag remains connected to the peritoneal catheter, is rolled up and held under a light waistband. After dwelling over night or for 4-6 hours during the day, the fluid is drained back into the empty bag, tis is discarded, a new dag is connected and fresh-dialysate runs into the abdomen. The exchange can be completed in 30 minutes. Continuous Cyclic Peritoneal Dialysis (CCPD) is a modification of CAPD, using an automated cycle to perform exchanges while the patient sleeps at night.
Advantages and disadvantages of CAPD
| Advantages | Disadvantages |
| No machine involved | Peritonitis due to contamination during bag exchange |
| No helper or nursing staff required | Time consuming for patients (4 exchanges at 30 min / 7 days a week) |
| Enhances mobility less cardiovascular stress. | Hyperlipidemia, hyperglycemia obesity |
| Maintains constant plasma solutes | Requires excess protein intake as 10-12 gm protein is lost daily. |
Contraindications of PD
Hyper catabolic state, serious arrhythmias
Diseases of abdominal wall or peritoneum
Respiratory insufficiency.
Possible indications for short term dialysis
Acute renal failure
Fluid overload
Uncontrolled hypercalcemia
Gross electrolyte disturbance
Poisoning with salicylates, barbiturates , ethanol
Acute on chronic renal failure prior to establishing conservative therapy.

Medlight2u
https://shorturl.fm/OI2SY
капельница от запоя клиника https://kapelnicza-ot-pokhmelya-samara-23.ru
mostbet table games mostbet94827.help
mostbet официальный mostbet официальный
1win бонус новым игрокам 1win бонус новым игрокам
Acne Acne vulgaris Acute Renal Failure Adrenal cortex Angina Angina Pectoris Aortic Regurgitation (AR) Aortic Stenosis (AS) Chest pain Chronic pyelonephritis Coarctation of Aorta Cough cyanosis Cystic acne Dehydration depression Diabetes Mellitus Diagnosis of Aortic Stenosis Dr.KTS DR K TAMILSELVAN Fatigue Heart Failure Hypertension Hypokalemia Hypothyroidism Ischemic Heart Disease LBBB Mitral Incompetence Mitral insufficiency Mitral valve prolapse Nocturia Patent Ductus Arteriosus PDA Polyuria Proteinuria pulmonary hypertension Pulmonary Stenosis ST Depression Symptoms of Acne Syncope Treatment for acne valvular heart disease Ventricular Septal Defect VSD Zits
Leave a Reply