Hyperoxaluria
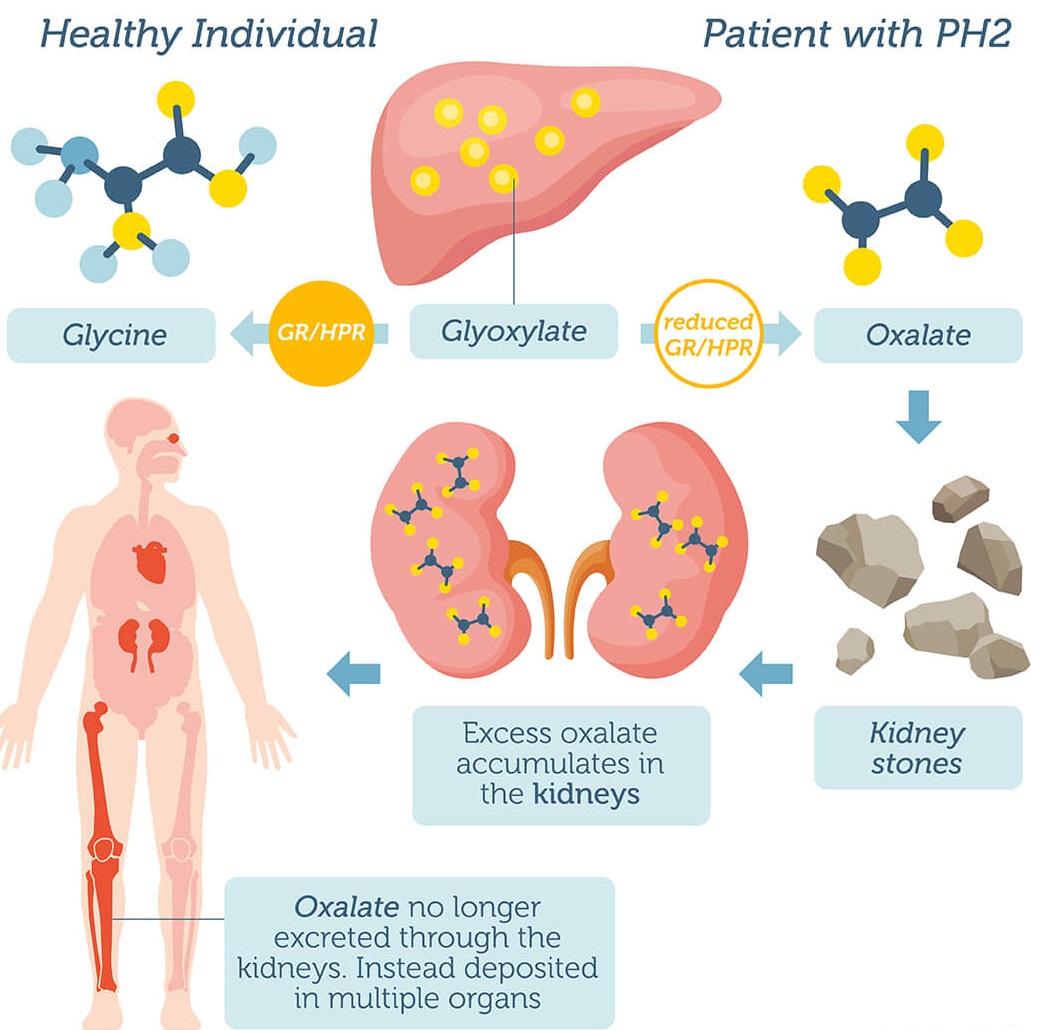
Primary hyperoxaluria is a rare condition characterized by the overproduction of a substance called oxalate (also called oxalic acid). In the kidneys, the excess oxalate combines with calcium to form calcium oxalate, a hard compound that is the main component of kidney stones. Deposits of calcium oxalate can lead to kidney damage, kidney failure, and injury to other organs.
Primary hyperoxaluria is caused by the shortage (deficiency) of an enzyme that normally prevents the buildup of oxalate. There are two types of primary hyperoxaluria, distinguished by the enzyme that is deficient. People with type 1 primary hyperoxaluria have a shortage of a liver enzyme called alanine-glyoxylate aminotransferase (AGXT). Type 2 primary hyperoxaluria is characterized by a shortage of an enzyme called glyoxylate reductase/hydroxypyruvate reductase (GRHPR).
Mostly autosomal recessive
Manifests in childhood with nephrolithiasis and oxalosis progressive to renal failure.
Increased serum glycolic acid and L-glyceric acid
Large doses of pyridoxine and high phosphate diet may enefit.
Calcium oxalate deposition occurs after renal transplant since there is defect in enzymes.
Some patients of pyridosine deficiency, chronic ileal disease, orotic aciduria, uricosturia and on drugs like acyclovir. NFT, SDZ and acetazolamide also have oxaluria.
Types of Hyperoxaluria
- Primary hyperoxaluria
- Enteric hyperoxaluria
- Idiopathic hyperoxaluria
- Oxalate poisioning
Treatment of Hyperoxaluria
The main therapeutic approach to primary hyperoxaluria is still restricted to symptomatic treatment, i.e. kidney transplantation once the disease has already reached mature or terminal stages. However, through genomics and proteomics approaches, efforts are currently being made to elucidate the kinetics of AGXT folding which has a direct bearing on its targeting to appropriate subcellular localization. Secondary hyperoxaluria is much more common than primary hyperoxaluria, and should be treated by limiting dietary oxalate and providing calcium supplementation. A child with primary hyperoxaluria was treated with a liver and kidney transplant. A favorable outcome is more likely if a kidney transplant is complemented by a liver transplant, given the disease originates in the liver.

medlight2u.com
Acne Acne vulgaris Acute Renal Failure Adrenal cortex Angina Angina Pectoris Aortic Regurgitation (AR) Aortic Stenosis (AS) Chest pain Chronic pyelonephritis Coarctation of Aorta Cough cyanosis Cystic acne Dehydration depression Diabetes Mellitus Diagnosis of Aortic Stenosis Dr.KTS DR K TAMILSELVAN Fatigue Heart Failure Hypertension Hypokalemia Hypothyroidism Ischemic Heart Disease LBBB Mitral Incompetence Mitral insufficiency Mitral valve prolapse Nocturia Patent Ductus Arteriosus PDA Polyuria Proteinuria pulmonary hypertension Pulmonary Stenosis ST Depression Symptoms of Acne Syncope Treatment for acne valvular heart disease Ventricular Septal Defect VSD Zits
Leave a Reply